Elaine Owen MBE MSc SRP MCSP Dip. Lower Limb Orthotic Biomechanics Dip. Clinical Gait Analysis ESMAC trained in Clinical Gait Analysis
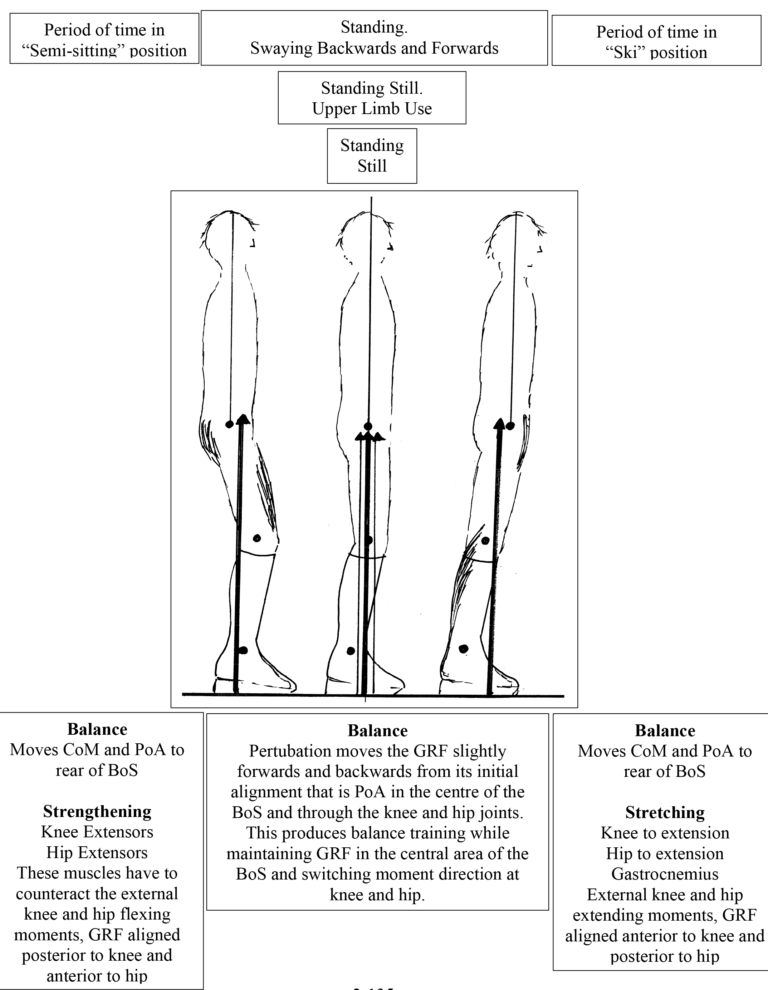
The Shank to Vertical Angle (SVA) alignment of the AFOFC will have been optimised by the therapist/orthotist. They will have chosen one that enables the thigh to become inclined. The design of the footwear will have also been optimised in regard to pitch, stiffness and profile, so that optimum heel and toe lever lengths are available for the exercise. Some children/adults will be able to do the exercise without physical help, as they will be able to keep the foot in total contact with the floor surface and therefore maintain the SVA that has been set for the exercise. Some children/adults will need some assistance to do this, either from equipment or from a person holding the upper shank as shown in figure B opposite.
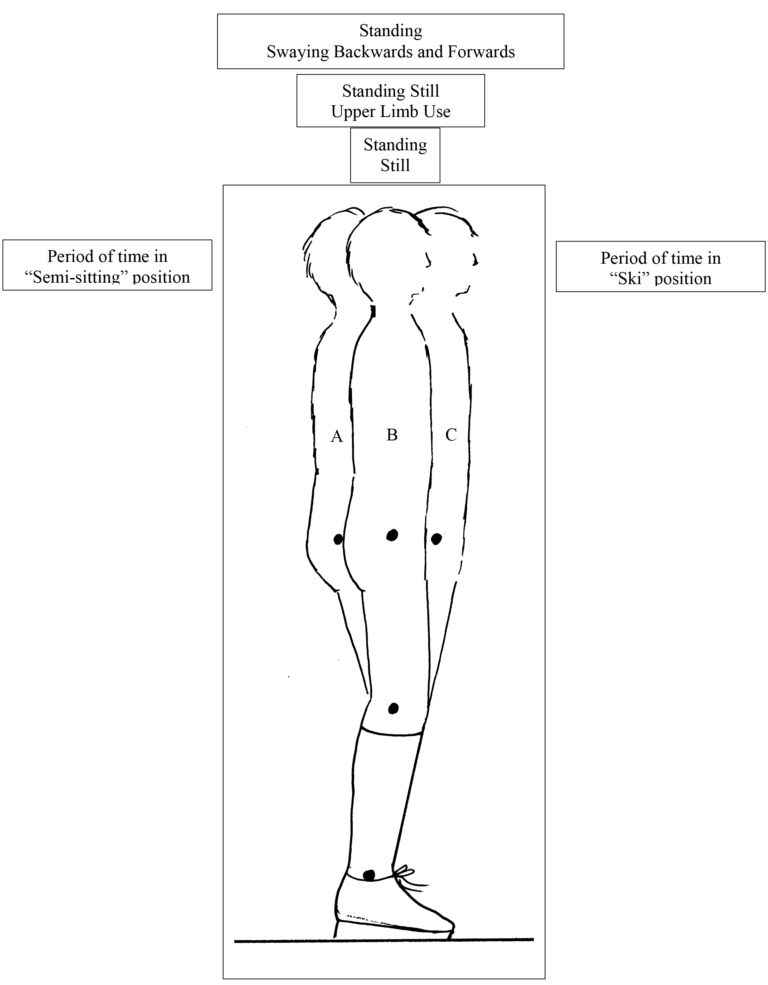
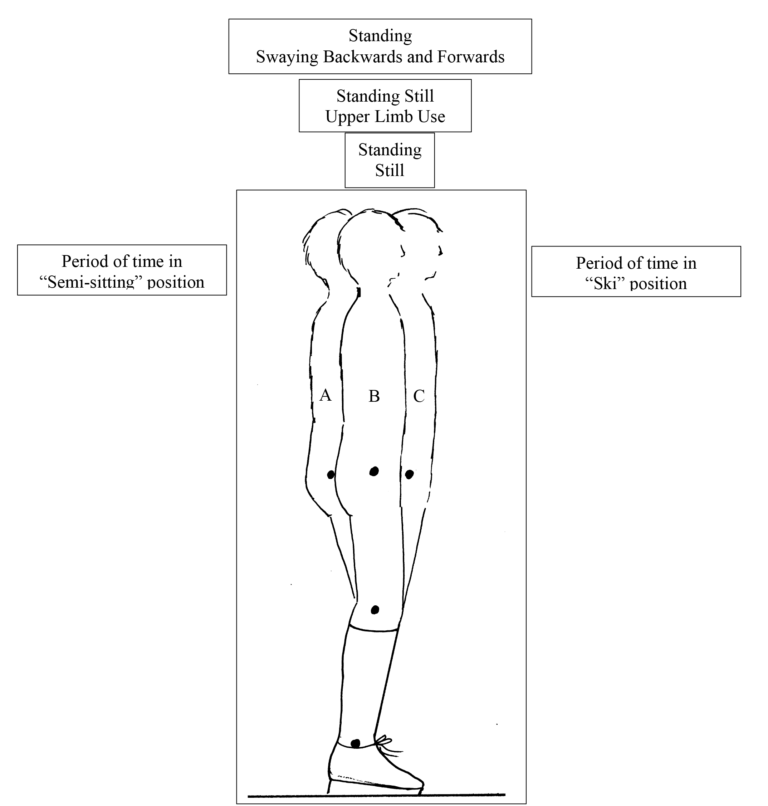
A B C
In standing, encourage the child to translate the trunk anteriorly and posteriorly, moving the thigh from a reclined to vertical and inclined position. Sustain A, B and C positions for the time set by therapist, repeating for the frequency set by therapist. Then progress to swaying between A and C, with the rhythm and timing set by therapist. The trunk ideally needs to remain vertical but if this is not possible this needs to be accepted and worked towards once the child has mastered the swaying and any obstructions to achieving vertical trunk alignment are reduced, for example joint ranges are increased. Physical prompts: The child may need support at the top of the shanks, to maintain the contact of the whole foot with the floor and the optimised SVA, as illustrated in C above. Physical prompts can be gradually reduced, or faded, as the child becomes more proficient at the exercise. For example if a strong hold is required initially it can be reduced gradually, to reach finally just a finger prompt and then no physical prompt at all. Verbal prompts: It is useful to use verbal prompts such as ‘ski’ ‘tuck bottom’ for C; ‘sit or ‘little sit’ for A; ‘bottom forward, bottom back’, at the required rhythm, for the swaying part of the exercise.
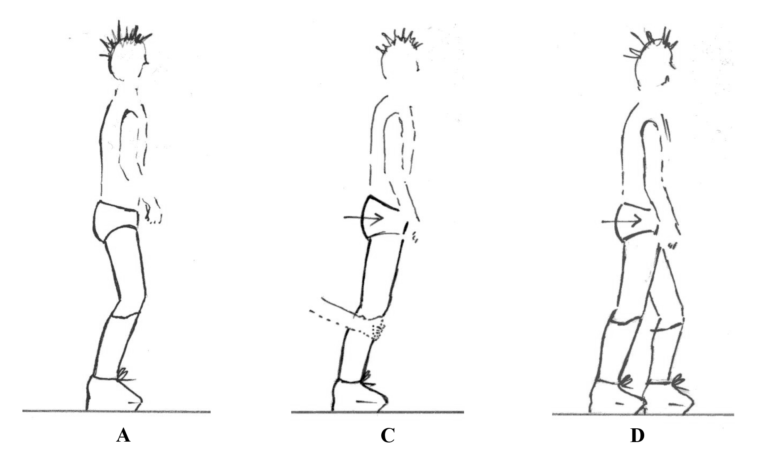
D
Step standing and stepping, with or without physical and verbal prompts as described above. Prompts can be reduced or faded as progress is made. Encourage small steps with the stance leg moving from an temporal MST position to an 40% GC position; foot can remain horizontal and in full contact with the floor, shank inclined, thigh inclined, when achieved the GRF will be aligned anterior to the knee and posterior to the hip, providing stabilising knee and hip extending moments.
References:
Owen E. (2016) Normal Gait Kinematics and Kinetics. Chapter 19 in Physical Therapy for Children with Cerebral Palsy; An Evidence-Based Approach. Editor; Mary Rahlin PT, DHS, PCS, Mary Franklin University, Chicago. Publisher Slack Incorporated.
Owen E. (2016) A Segmental Kinematic Approach to Orthotic Management: Ankle-Foot Orthosis/Footwear Combination. Chapter 21 in Physical Therapy for Children with Cerebral Palsy; An Evidence-Based Approach. Editor; Mary Rahlin PT, DHS, PCS, Mary Franklin University, Chicago. Publisher Slack Incorporated.
Owen E and Ivanyi B. (Due publication 2016) Chapter ‘Spina Bifida in Children. Directives for Footwear and AFO Footwear Combinations’. In: Orthopaedic and Pedorthic Footwear. Assessment, Indications and Treatment plans. Editor Klaas Postema, Netherlands.
Owen E (2014) From stable standing to rock and roll walking (Part 2). Designing, Aligning and Tuning for Standing, Stepping and Gait. Submitted to Association of Paediatric Chartered Physiotherapists Journal
Owen E (2014) From stable standing to rock and roll walking (Part 1) The importance of alignment, proportion and profiles. Association of Paediatric Chartered Physiotherapists Journal 5 (1): 7-18
Owen E (2013) A proposed clinical algorithm for dorsiflexion free AFO footwear combinations based on calf muscle length, strength, stiffness and skeletal alignment. ISPO UK NMS Scientific Meeting 2013, BLESMA prize award.
Owen E (2010) The importance of being earnest about shank and thigh kinematics especially when using AFOs. Prosthetics and Orthotics International Sept 34(3): 254-269.
Owen E (2009) How should we define the rockers of gait and are there three or four. Gait & Posture. 30S:S49
Meadows CB, Bowers R, Owen E (2008) Chapter 22 “Biomechanics of Hip Knee and Ankle” In: American Academy of Orthopaedic Surgeons, Atlas of Orthoses and Assistive Devices, Elsevier
Owen E (2005) A clinical algorithm for the design and tuning of ankle-foot orthosis footwear combinations (AFOFCs) based on shank kinematics. Gait & Posture 22S: S36-S37
Owen E (2005) Proposed clinical algorithm for deciding the sagittal angle of the ankle in an ankle-foot orthosis footwear combination. Gait & Posture 22S: S38-S39
Owen E (2004) “Shank angle to floor measures” and tuning of “Ankle-foot orthosis footwear combinations” for children with cerebral palsy, spina bifida and other conditions. MSc Thesis. Glasgow: University of Strathclyde. Available from lugger@talk21.com
Owen E (2002) Shank angle to floor measures of tuned ‘ankle-foot orthosis footwear combinations’ used with children with cerebral palsy, spina bifida and other conditions. Gait & Posture 16: Supp 1, S132-S133